Gynecomastia — male breast enlargement, and why the answer is found by hand
Gynecomastia is a benign enlargement of the glandular tissue of the male chest, driven by a shift in the balance between estrogen and testosterone. Male breast cancer is a different disease — but from the outside, in the mirror, both begin as a swelling. That is the whole problem, and it is why this guide ends where it must: in an examination room. Dr. Khaled Ghalwash examines the chest, grades it, and only then names the operation.
Most men arrive with the same two questions, and this page takes both seriously. It will not answer either from a photograph — but it will tell you exactly how each one is answered, and where the honest answer is found.
The two questions every man arrives with
They are almost always these, in these words: “هو ليه صدري كبر؟” — why did my chest grow? — and “هو ممكن يكون ورم خبيث؟” — could it be malignant? Both are good questions. The second one is the one that must be answered first, because it changes how urgently you are seen. Neither can be answered by a photograph, a search result, or this page — but each has an honest path, and both paths run through the same examination.
Start where your worry is: could it be cancer, or why did my chest grow.
What gynecomastia actually is — and what it is not
Gynecomastia is the growth of the glandular tissue of the male breast, caused by a relative rise in estrogen compared with testosterone. It is benign. Two facts about its relationship to cancer are worth stating precisely, because they are often twisted in both directions. First: gynecomastia does not turn into cancer — the tissue does not transform. Second: men with gynecomastia may carry a slightly higher lifetime risk of male breast cancer — not because the gland becomes malignant, but because the hormonal imbalance that causes the one is itself a risk factor for the other. Neither sentence is a reason to panic, and neither is a reason to relax.
Gland, fat, or both
Not every enlarged male chest is the same tissue. Some is fatty (pseudogynecomastia), some is a true firm glandular disc behind the nipple, and most — in practice — is a mixture of both. The distinction is not academic: it is what decides whether the problem shrinks with weight loss, and whether an operation can be done by suction alone or must also remove the gland. It cannot be settled in a mirror, because fat and gland look identical from the outside and feel completely different under the fingers. Why did my chest grow · VASER and gland excision.
The four features that separate them
Benign gynecomastia tends to be soft and rubbery, centred directly beneath the nipple, often on both sides, with normal skin and a normal nipple. Male breast cancer tends to be hard and irregular, off-centre, almost always one-sided, and may change the skin or pull the nipple in. But these are the features a trained hand reads against the chest wall — a firm gland and a firm cancer can feel the same to your own fingers. The full comparison, the warning signs, and what to do about each are on the cancer page. Could it be cancer →
The four questions, answered properly

Dr. Khaled Ghalwash examines every male chest himself before he says a word about surgery. The examination is not a formality before the operation — it is the diagnosis, it is the grading, and it is what chooses the technique. A man who is told his operation over the phone has not been diagnosed.
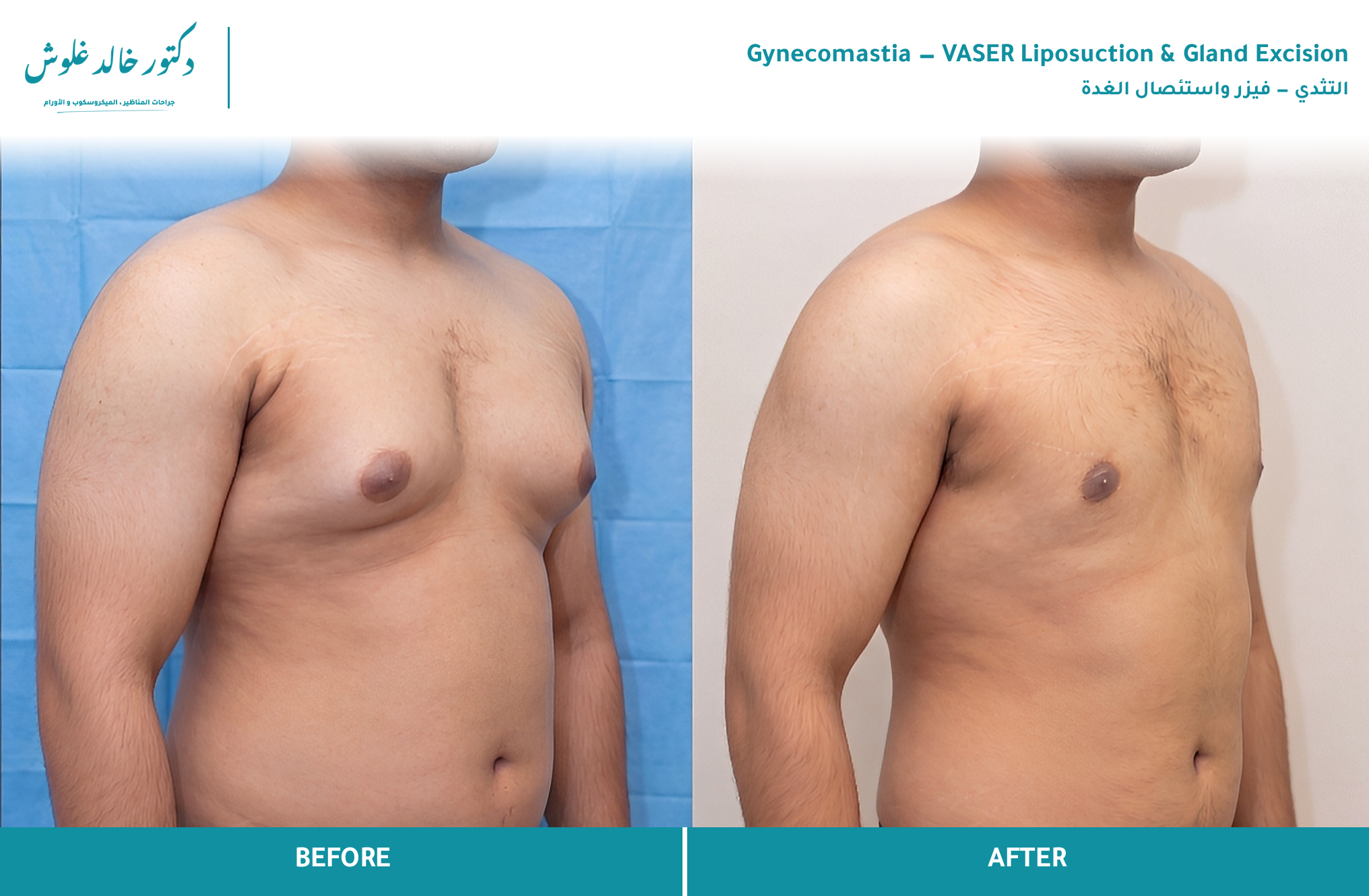
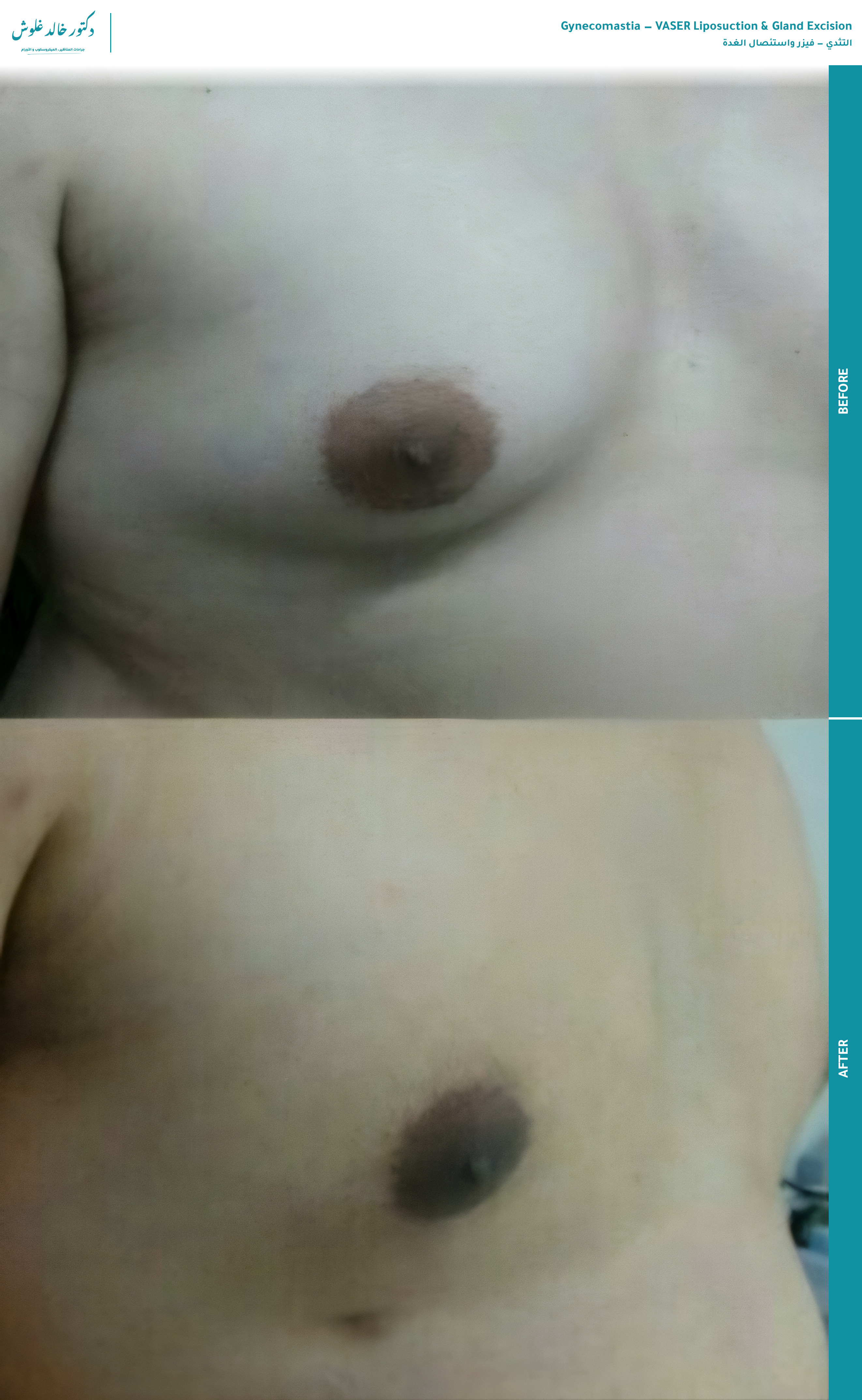
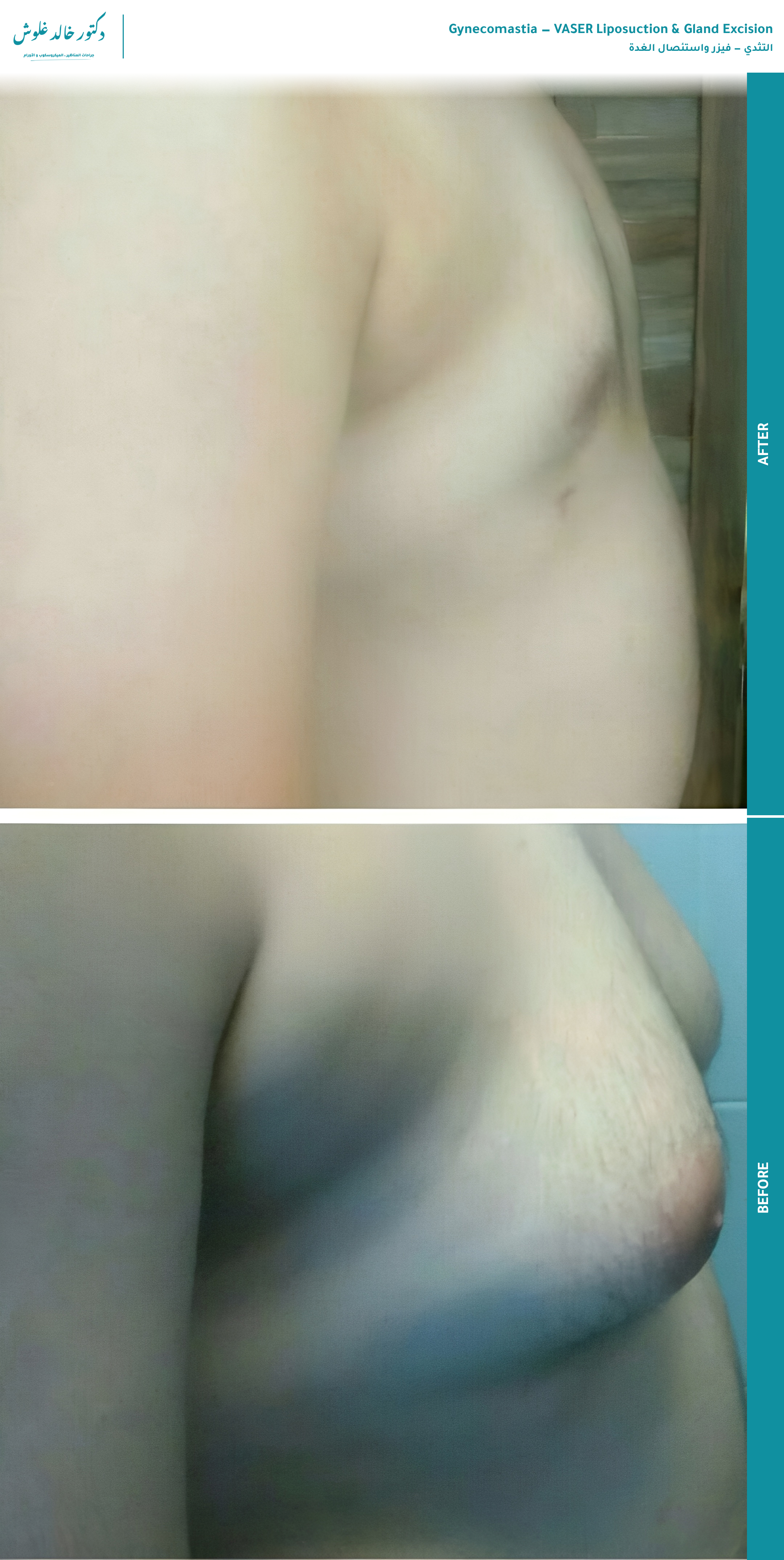
Results
Consented before-and-after cases. Each links to the full case in the results gallery.

Frequently asked questions
Why did my chest grow?
Gynecomastia is a benign enlargement of the glandular tissue of the male chest, driven by a shift in the balance between estrogen and testosterone — not by a single "level" being wrong. A medication, a steroid cycle, a liver or thyroid problem, a genetic condition, or a stage of life can all tip that balance. Knowing which one started it matters for treatment, but it does not tell you what the tissue is. Why did my chest grow →
Could it be malignant — could it be cancer?
Almost always, no. Gynecomastia is benign and it does not turn into cancer. But male breast cancer is a separate disease that also begins as a chest swelling, and "almost always" is not a diagnosis — which is why it cannot be settled from a photograph or a web page, and why I will not give you a verdict over a screen. Could it be cancer →
I am embarrassed to be examined. Is there any way to know without it?
No — and this is the honest answer that matters most. Texture, the exact position of the swelling under the nipple, and whether it is gland or fat are read by hand against the chest wall. A photograph cannot show any of them. The examination is short, it is the chest only, and it is over quickly. Embarrassment is the single most common reason men arrive late with something that would have been simpler to treat earlier.
Will it go away on its own, or do I need surgery?
It depends on what caused it and how long it has been there. Recent, drug-induced enlargement can settle when the cause is removed. Long-standing tissue that has become firm and fibrous usually does not, and a true glandular disc does not shrink with weight loss or exercise. Which of these you have is an examination finding, not something you can judge from the outside.
Does this mean my hormones are broken, or that I am less of a man?
No. Gynecomastia is common and it reflects a ratio between two hormones, not a failure of manhood. In many men the trigger is temporary or external — a medication, a supplement, a phase of life — and the chest itself is a mechanical problem that is corrected mechanically. It is not a judgement on you.
If I lose weight or train, will the chest shrink?
Fat responds to weight loss and training; the gland does not. If your enlargement is mostly fat (pseudogynecomastia), losing weight helps. If there is a true glandular disc behind the nipple, it stays — and chest exercises can even push it forward and make it more obvious. Telling fat from gland is exactly what the examination does.
Will the surgery leave a visible mark?
The technique used keeps the scar within the colour border of the areola, where it is hard to see once healed — no vertical scar and no horizontal scar across the chest. The exact plan depends on how much skin is involved, which is decided at the examination. VASER and gland excision →
The one thing a web page cannot do
It cannot examine you. The examination is what tells benign from suspicious, gland from fat, and which operation — if any — you need. Book it, and you will be told plainly what your chest is.
The examination →