VASER and gland excision — the two halves of a gynecomastia operation
VASER emulsifies fat with ultrasound before it is aspirated, which is what makes a smooth, even male chest contour possible. What VASER cannot do is remove the gland — the firm disc behind the nipple is fibrous and it does not emulsify. It has to be cut out. And once it is out, whatever skin was holding it has to go somewhere. Those three facts — fat, gland, skin — are the whole operation.
Two tissues, two instruments
A male chest that has grown is rarely one tissue. There is fat, which is soft and spread over the whole chest, and there is gland — a firm, fibrous disc that sits directly behind the nipple. Male fat is denser and more fibrous than the fat of a female body, which is why it needs a tool that can break it up evenly rather than drag through it. VASER — ultrasound-assisted liposuction — emulsifies that fat before it is aspirated, which is exactly right for the fatty compartment. It is exactly wrong for the gland: ultrasound will not turn a fibrous disc into something that can be suctioned.
The art of using VASER on a male chest
The skill is not in how much fat is removed — it is in where the transition sits. Energy is delivered in the plane of the fat, not against the underside of the skin, so the surface stays even. The male chest is judged on its borders more than its volume: the goal is a smooth, tapered transition into the fold of the armpit and along the lower line of the chest, so the eye reads a flat plane rather than an edge. The classic failure is the opposite — too much taken centrally, under the nipple, and too little at the borders, which leaves a hollow that reads as worse than the chest the man started with. Restraint at the centre and blending at the edges is the whole craft, and it is judgement, not force.
Why the gland has to come out separately
The glandular disc is fibrous and anchored behind the nipple, and suction — however good — leaves it behind. It is removed directly, through the border of the areola, as a separate step from the liposuction. This is why one of the most common reasons men come for a second opinion is a chest that had liposuction alone: the fat went, but the firm disc under the nipple stayed, and it is still palpable and still visible. Correcting that means excising the residual gland that should have come out the first time. Revision surgery →
And then the skin
Once the fat and the gland are gone, the skin that was holding them has to take up the slack. When there is only mild redundancy, the skin retracts on its own and nothing further is needed. When there is more, it does not — and this is the point at which many operations reach for a vertical or horizontal scar across the chest. The technique below is how that redundancy is managed without one.
The technique: an eccentric periareolar crescentic excision
In the reconstructive surgery literature, this geometry is classified as an eccentric periareolar crescentic excision — and it is built to correct skin redundancy while keeping every scar inside the border of the areola. It works through two opposing crescents:
- An infero-medial half-circle, one centimetre wide, is de-epithelialized — the epidermis is removed but the dermis is kept. That preserved dermis carries the subdermal blood supply and the nerves of the nipple-areola complex: it is a de-epithelialized dermal pedicle, and it is why the nipple keeps both its blood supply and its sensation.
- An upper-lateral half-circle, one centimetre wide, is cut full-thickness — this is the excision that creates the void and gives access to the gland.
- On closure, the nipple-areola complex advances superolaterally over the de-epithelialized bed. The redundant skin is taken up, and the scar lies entirely within the colour border of the areola.
This is deliberately not a concentric (round-block / Benelli) design, which de-epithelializes a full 360-degree ring and relies on a purse-string suture to gather redundancy all the way around. The eccentric crescent gives a directional lift instead — which is what actually corrects the infero-medial droop that gynecomastia tends to produce — and, by confining the de-epithelialization and the full-thickness cut to opposing crescents, it puts far less radial tension on the closure. Lower tension is what protects against the areola spreading and against a raised, thickened scar. The net effect is that skin redundancy is treated with no vertical and no horizontal scar on the chest.
The operation in four steps
-
1
Mark upright
The crescents are drawn with the patient standing, before anaesthesia — because skin redundancy only shows against gravity.
-
2
VASER the fat
Ultrasound emulsification and aspiration of the fatty compartment, blended into the borders of the chest and the axillary fold.
-
3
Excise the gland
The glandular disc is removed directly through the upper-lateral full-thickness crescent, leaving a deliberate cuff of tissue beneath the areola so the nipple does not sink.
-
4
Advance and close
The nipple-areola complex is advanced superolaterally over the de-epithelialized dermal bed, and the closure is kept within the areolar border.
Three tissues, three problems, three answers
| The problem | Fat | Gland | Skin |
|---|---|---|---|
| What it is | Soft, diffuse, over the whole chest | Firm fibrous disc behind the areola | The envelope that held both |
| Does VASER treat it? | Yes — emulsified, then aspirated | No — it does not emulsify | No |
| What treats it | VASER liposuction | Direct excision through the areolar border | Retraction if mild; eccentric periareolar crescentic excision if not |
| What decides it | Examination | Examination | Examination |
What the scar actually is
The scar sits within the colour border of the areola, where the transition from areola to skin hides it. There is no vertical scar and no horizontal scar across the chest. Like any scar it is visible while it matures and fades over the following months; the aim is a chest that reads as a normal male chest rather than one that looks operated on.
Recovery
A compression garment is worn after surgery to support the chest and help the skin settle onto its new contour. Light, desk-type activity is resumed early; heavier training and chest work are reintroduced gradually as healing allows. The exact timeline depends on how much was done, and it is given to you at the examination rather than promised in advance. Swelling and bruising are expected in the first weeks and settle as the final contour appears.
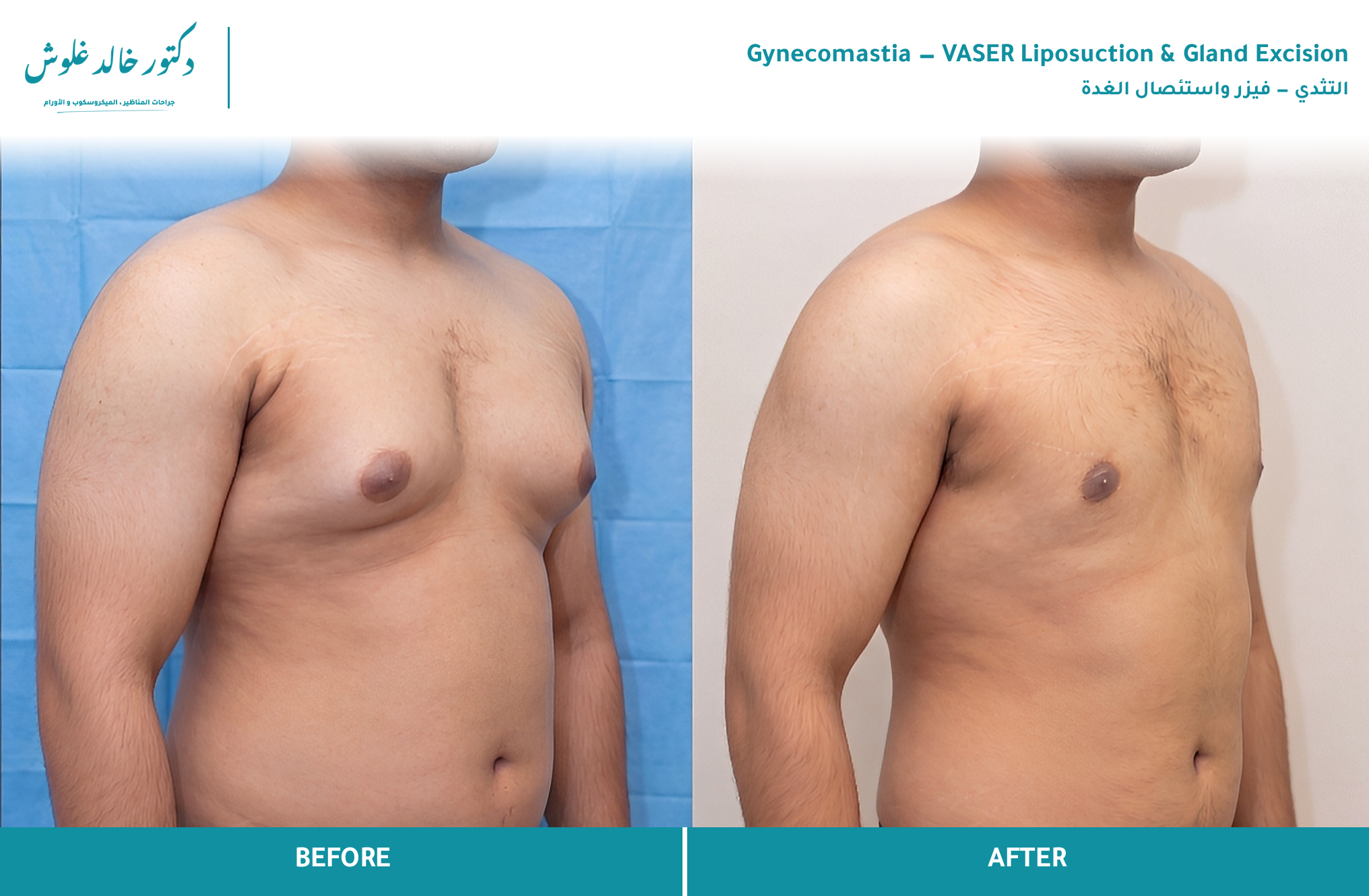
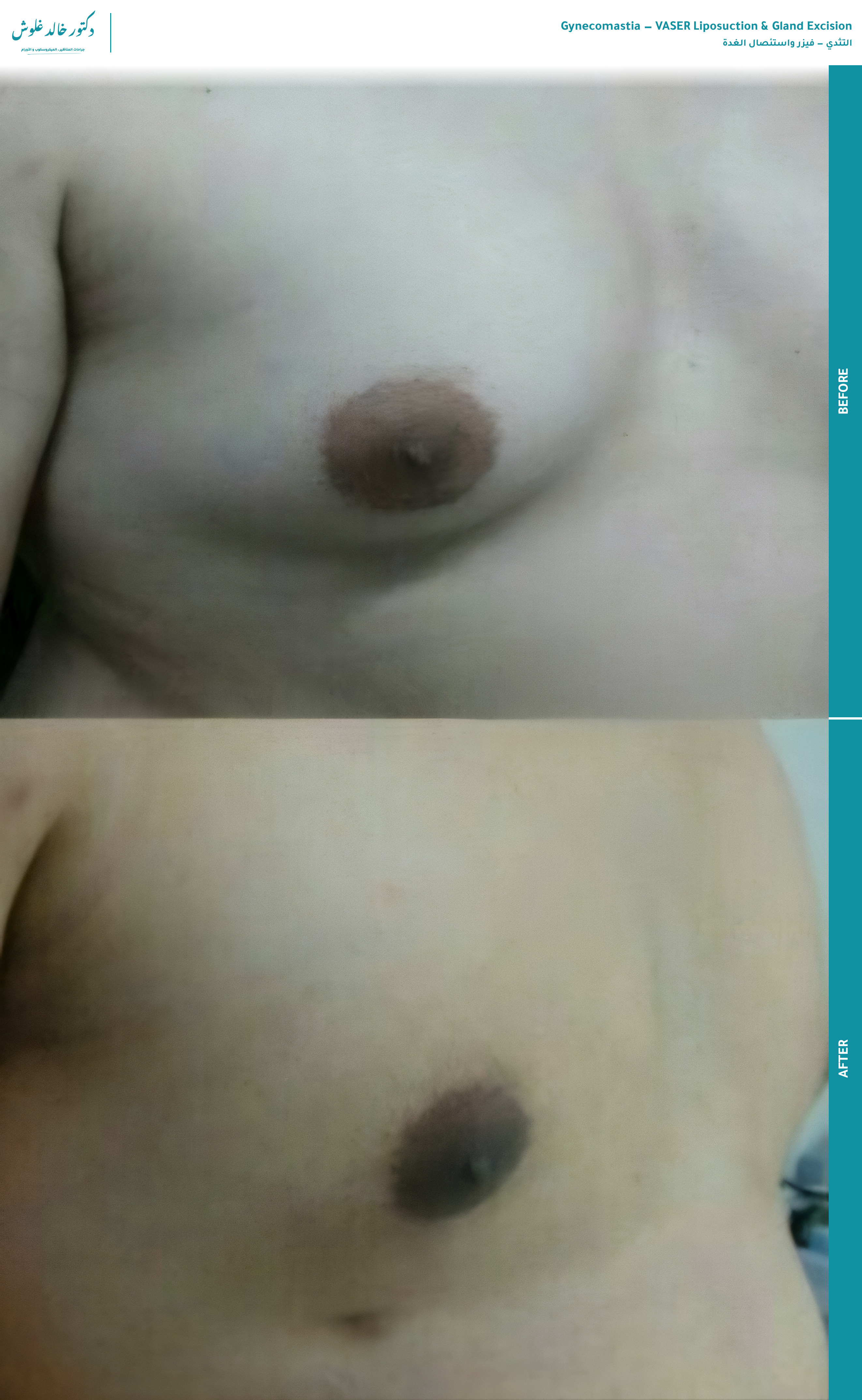
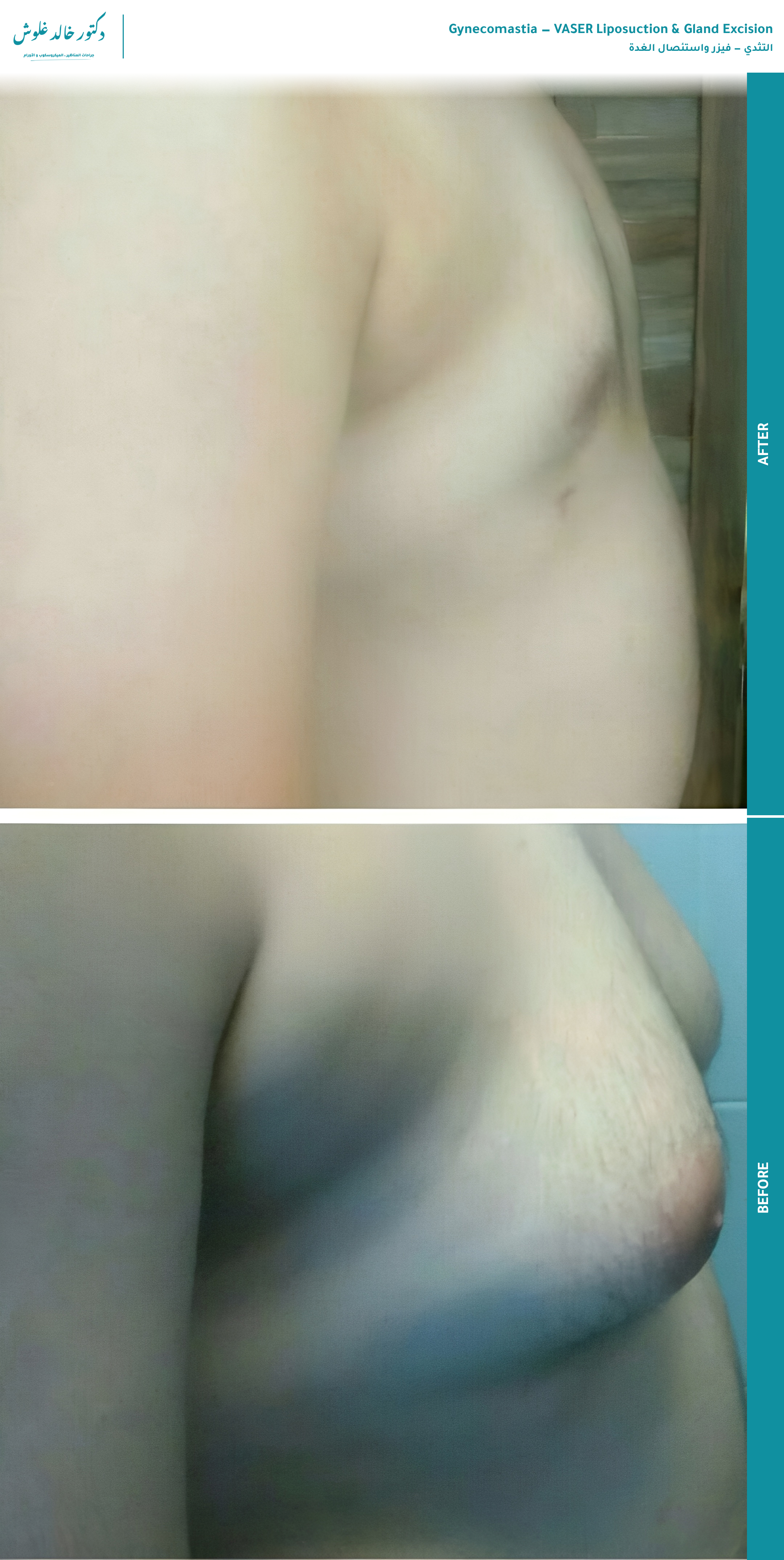
Results
Consented before-and-after cases. Each links to the full case in the results gallery.

Frequently asked questions
Can I have VASER only, with no cutting?
Only if there is no gland. VASER emulsifies and removes fat beautifully, but the firm glandular disc behind the nipple does not emulsify — suction alone leaves it behind. Whether your chest is fat, gland, or both is an examination finding, not a preference, and it is the single fact that decides whether VASER alone can work.
Will it leave a mark? Will people at the gym know?
The scar is placed within the colour border of the areola, where it is hard to see once healed — there is no vertical scar and no horizontal scar across the chest. The aim is a chest that simply looks like a normal male chest, not one that looks operated on.
Will my nipple still have sensation?
The technique is built specifically to protect it. The de-epithelialized crescent preserves the dermis beneath the areola, and with it the blood supply and the nerves that give the nipple its sensation. Sensation is protected by design rather than left to chance — the exact expectation for your case is discussed at the examination.
Can it come back after surgery?
Glandular tissue that is excised does not grow back. Fat can return with significant weight gain, and if the original cause returns — a steroid cycle, for instance — the process can restart. This is why the cause is addressed alongside the operation. Why it happened →
I had surgery before and there is still something firm — can it be fixed?
Yes — this is one of the commonest reasons men come for a second opinion: liposuction was done but the glandular disc was left behind, so a firm lump remains under the nipple. Correcting it means excising the residual gland directly and evening out the contour. Revision surgery →
How many days off, and when can I train again?
A compression garment is worn after surgery and desk-type work is resumed within a few days; heavier training and chest work are reintroduced gradually once healing allows. The exact timeline depends on the extent of the operation and is given to you at the examination rather than promised in advance.
Will there be a drain? A compression garment?
A compression garment is standard — it supports the chest and helps the skin settle onto the new contour. Whether a drain is used depends on the extent of the gland removed and how much space is left behind; it is decided during the operation and explained to you beforehand.
The technique is chosen at the examination, not before it
Which operation is right — and whether the skin needs the crescent technique at all — is decided by what the examination finds, not from a photograph. Book it, and the plan is drawn for your chest specifically.
The examination →